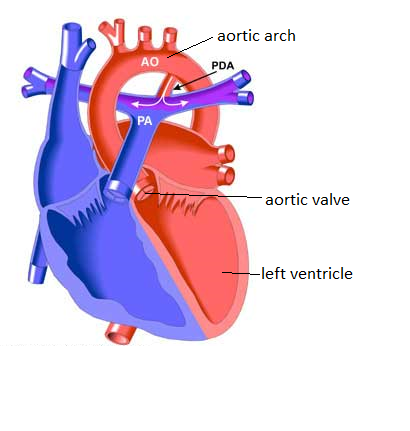
Healthy Heart ReviewWhen the left ventricle contracts, blood shoots through the aortic valve and into the aorta (AO). The blood then travels through the aortic arch, which branches at the apex to feed the head and arms, and descends on to the rest of the body.
Ductus arteriosus- in a fetus, there is a passageway at the top of the descending aorta that connects it to the pulmonary artery (PA). This allows blood to bypass the lungs, which are not yet operational, and continue on to circulate throughout the body. |
Retrieved from http://www.pted.org/?id=patentductus1
|
Coarctation of the Aorta (CoA)
 Retrieved from http://www.chw.org/~/media/Images/MedicalCare/HeartCare/Conditions/
img_coar_heart.gif
Retrieved from http://www.chw.org/~/media/Images/MedicalCare/HeartCare/Conditions/
img_coar_heart.gif
What is it?
A Coarctation of the Aorta (CoA) is a narrowing of the aorta that occurs typically in the descending aortic arch, just after the point where the three branches supplying blood to the head and arms branch off. A CoA can range in severity from a mild narrowing to severe restriction.
What causes it?
It is not known for certain what causes CoAs to form, and at this time, it cannot be diagnosed with certainty prenatally. It is also frequently missed in initial exams by healthcare professionals, leading to increased risk for morbidity and mortality.
How does it affect the body?
A CoA will cause the heart to work significantly harder in order to push blood through the narrowed opening in the aorta. If this continues for an extended period of time, the build of up blood in the heart, and the extra strain could lead to Congestive Heart Failure. Blood that is backed up behind the area of the CoA also causes a significant increase in blood pressure in the upper extremities and head. Blood flow past the CoA will be greatly decreased, causing low blood pressure and flow in the mid-section and lower extremities. Typically, symptoms worsen after the closure of the ductus arteriosus, and the body develops alternate pathways called collaterals to supply the lower body with adequate blood supply. These collaterals will enlarge the longer a CoA goes undetected.
A Coarctation of the Aorta (CoA) is a narrowing of the aorta that occurs typically in the descending aortic arch, just after the point where the three branches supplying blood to the head and arms branch off. A CoA can range in severity from a mild narrowing to severe restriction.
What causes it?
It is not known for certain what causes CoAs to form, and at this time, it cannot be diagnosed with certainty prenatally. It is also frequently missed in initial exams by healthcare professionals, leading to increased risk for morbidity and mortality.
How does it affect the body?
A CoA will cause the heart to work significantly harder in order to push blood through the narrowed opening in the aorta. If this continues for an extended period of time, the build of up blood in the heart, and the extra strain could lead to Congestive Heart Failure. Blood that is backed up behind the area of the CoA also causes a significant increase in blood pressure in the upper extremities and head. Blood flow past the CoA will be greatly decreased, causing low blood pressure and flow in the mid-section and lower extremities. Typically, symptoms worsen after the closure of the ductus arteriosus, and the body develops alternate pathways called collaterals to supply the lower body with adequate blood supply. These collaterals will enlarge the longer a CoA goes undetected.
|
How can I assess for it?
Often, symptoms do not appear until the closure of the ductus arteriosus, and still may not be detectable if the CoA is very mild. In 25% of cases, the CoA is severe enough that the neonate will go into heart failure and shock shortly after the closure of the ductus arteriosus. These babies will display:
|

Retrieved from https://neonatalcapstone.files.wordpress.com/2011/03/pg_neonate_sup0904_main.jpg
http://www.pted.org/pics/pda1.jpg
|
How can it be treated?
Surgery is the standard treatment option for a person with a CoA, in which the area of the CoA is cut out, and the aorta sewn back together above and below the affected area. A balloon angioplasty, where a catheter is inserted and dilated, is occasionally performed, though this method is more typical in cases of recoarctation, and can cause several complications on a native coarctation.
Surgery is the standard treatment option for a person with a CoA, in which the area of the CoA is cut out, and the aorta sewn back together above and below the affected area. A balloon angioplasty, where a catheter is inserted and dilated, is occasionally performed, though this method is more typical in cases of recoarctation, and can cause several complications on a native coarctation.
