|
While there are many CHDs that do not pose significant problems to the infant's growth and development, critical CHDs pose a significant threat to morbidity and mortality if not detected shortly after birth. While it is increasingly possible to find and detect cardiac birth defects prenatally, most are diagnosed after delivery. Many newborns suffering from critical CHDs do not exhibit noticeable symptoms until the ductus arteriosus begins to close. One in three cases of critical CHD is not detected before the infant's hospital stay is over. It is therefore critical to assess all seemingly healthy newborns for these defects before they leave the hospital.
|

Retrieved from http://baby.more4kids.info/2008/12/benefits-of-swaddling-your-baby/
|
Inspection
It is always important to start a nursing assessment with inspection. Not the general appearance of the infant. The nurse should note the color of the infant's skin. Central cyanosis is assessed around the oral mucosa of the infant, while peripheral cyanosis is seen in the hands and feet. Peripheral cyanosis is typically attributable to vasomotor instability or cold stress, while central cyanosis is normally attributable to a more sinister cause. If an infant presents with cyanosis, a hyperoxia test may be performed to rule out respiratory issues. When oxygen is applied to the infant, oxygen saturation and cyanosis will improve if the cause is respiratory or solely left to right shunting. If symptoms do not improve, further evaluation is needed to assess cardiac function. The nurse should also assess how hard the infant is having to work to breath. Signs of respiratory distress such as tachypnea, retractions, grunting, and nasal flaring are late indicators of cardiac failure as a result of pulmonary edema secondary to inadequate ventricular emptying or overload. Mottling of the skin may also occur with decreased peripheral perfusion and should be assessed for by the nurse.
It is always important to start a nursing assessment with inspection. Not the general appearance of the infant. The nurse should note the color of the infant's skin. Central cyanosis is assessed around the oral mucosa of the infant, while peripheral cyanosis is seen in the hands and feet. Peripheral cyanosis is typically attributable to vasomotor instability or cold stress, while central cyanosis is normally attributable to a more sinister cause. If an infant presents with cyanosis, a hyperoxia test may be performed to rule out respiratory issues. When oxygen is applied to the infant, oxygen saturation and cyanosis will improve if the cause is respiratory or solely left to right shunting. If symptoms do not improve, further evaluation is needed to assess cardiac function. The nurse should also assess how hard the infant is having to work to breath. Signs of respiratory distress such as tachypnea, retractions, grunting, and nasal flaring are late indicators of cardiac failure as a result of pulmonary edema secondary to inadequate ventricular emptying or overload. Mottling of the skin may also occur with decreased peripheral perfusion and should be assessed for by the nurse.

Retrieved from http://clinicalgate.com/cardiovascular-assessment-of-infants-and-children/
|
Palpation
The nurse should palpate peripheral pulses and pay attention to the rate, rhythm, quality, and compare the pulses between the upper and lower extremities. Sometimes, palpable thrills can be felt in patients with CHD. The nurse can palpate the infant at the precordium to assess for these. They will feel similar to a cat purring, and can be felt better when palpated with the finger tips. The nurse should also palpate the infant's skin to assess for moisture and temperature. |
Auscultation
When auscultating the heart, the nurse should listen for the first (S1) and second (S2) heart sounds, as well as any other sounds that might be present. Heart murmurs are the result of turbulent blood flow through the chambers of the heart, which the nurse should listen for when performing a cardiac assessment. The ductus arteriosus will often cause a murmur to be heard in the heart, but once it closes, murmurs indicate a an underlying cardiac malformation 54% percent of the time and are usually associated with S2 heart sounds. All heart murmurs should therefore be monitored and reported, but the nurse should also be aware that infants may not have a murmur even in the presence of critical CHD.
When auscultating the heart, the nurse should listen for the first (S1) and second (S2) heart sounds, as well as any other sounds that might be present. Heart murmurs are the result of turbulent blood flow through the chambers of the heart, which the nurse should listen for when performing a cardiac assessment. The ductus arteriosus will often cause a murmur to be heard in the heart, but once it closes, murmurs indicate a an underlying cardiac malformation 54% percent of the time and are usually associated with S2 heart sounds. All heart murmurs should therefore be monitored and reported, but the nurse should also be aware that infants may not have a murmur even in the presence of critical CHD.
|
Blood Pressure
When taking an infant's blood pressure, it is important to begin with the correct cuff size in order to obtain an accurate reading. The blood pressure should be taken from the infant's right arm, and one of the infant's legs to be compared against one another. Significant differences between the extremities could indicate a defect along the aortic arch. Blood pressure will be the last vital sign to indicate that an infant is in trouble. The nurse should also assess the infant's peripheral pulses including radial, posterior tibial, and femoral, paying attention to rate, rhythm, character, and equality to one another. Weak pulses could be a sign of poor perfusion, and differences between upper and lower body could again be a sign that the infant has a coarctation. The nurse should also assess capillary refill time by pressing down on a bony area and counting the seconds it takes for the skin to return to full color. A normal reperfusion is under 3 seconds. |
Cardinal Signs of Congenital Heart Disease:
|
 Retrieved from http://www.sciencedirect.com.byui.idm.oclc.org/science/article/pii/
S0884217515315525
Retrieved from http://www.sciencedirect.com.byui.idm.oclc.org/science/article/pii/
S0884217515315525
Pulse Oximetry
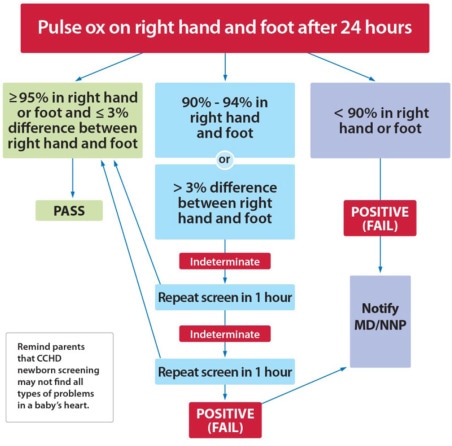
Pulse oximetry is a noninvasive method that can be used to detect invisible hypoxia resulting from critical heart defects. It should be measured after the infant has reached 24 hours in age, or as late as possible before discharge, to prevent potential false positives resulting from a patent ductus arteriosus, and detect potential ductal dependent lesions. Probes are placed on the infant's right hand (preductal, or proximal part of the aorta in relation to ductus arteriosus) and either foot (postductal, distal part of aorta in relation to ductus arteriosus). An infant passes if one of the readings in the hand or foot is >95, and there is <3% difference between the readings. This finding indicates that it is unlikely that the infant has a critical CHD. Findings below or equal to 90 should be immediately reported to the provider for follow-up. For readings of 90 to 95, or if the difference between the readings is >3%, a retest should be done an hour later. If results are still inconclusive, another retest should be done in another hour. To the left is the algorithm that should be followed when using pulse oximetry to test infants for critical CHDs. It should be noted that pulse oximetry screening does not detect all cardiac defects, and therefore the nurse's physical assessment is still very important.
Pulse oximetry is a noninvasive method that can be used to detect invisible hypoxia resulting from critical heart defects. It should be measured after the infant has reached 24 hours in age, or as late as possible before discharge, to prevent potential false positives resulting from a patent ductus arteriosus, and detect potential ductal dependent lesions. Probes are placed on the infant's right hand (preductal, or proximal part of the aorta in relation to ductus arteriosus) and either foot (postductal, distal part of aorta in relation to ductus arteriosus). An infant passes if one of the readings in the hand or foot is >95, and there is <3% difference between the readings. This finding indicates that it is unlikely that the infant has a critical CHD. Findings below or equal to 90 should be immediately reported to the provider for follow-up. For readings of 90 to 95, or if the difference between the readings is >3%, a retest should be done an hour later. If results are still inconclusive, another retest should be done in another hour. To the left is the algorithm that should be followed when using pulse oximetry to test infants for critical CHDs. It should be noted that pulse oximetry screening does not detect all cardiac defects, and therefore the nurse's physical assessment is still very important.
